
DESTINY-Breast 03 - The rise of the ADC
For those unfamiliar with the world of Destiny trials, these trials were created to see whether T-DXd (trastuzumab deruxtecan), an antibody-drug conjugate, could be another treatment option for patients with HER-2 positive cancers, and what a whirlwind it has been. Cancer types targeted include breast, lung, gastric and colorectal cancer, to name a few (1). Most recently, DESTIY-Breast06 was presented at ASCO 24, confirming that enhertu (T-DXd) has significant and clinically meaningful activity in the HER-2 low metastatic breast cancer cohort of patients for progression-free survival, antitumour activity and a numerical benefit for overall survival (data is still immature) (2). This will change the landscape of breast cancer treatment for years to come. This article takes a step back and looks at the big brother DESTINY-Breast03, which is no less critical. This trial was positioned to see whether T-DXd was superior to trastuzumab emtansine (TDM-1) as a second-line therapy post-progression on trastuzumab with a taxane.
As a background, breast cancer is the most commonly diagnosed cancer and also the most lethal to women worldwide. However, this varies depending on access to screening, treatment and prevention practices (4). HER-2 expression is found in approximately 20% of breast cancers, and while treatment has exponentially improved over the last 15 years, more is needed for those who relapse or progress (5,6). Historically, HER-2 cancers were considered very aggressive, metastasise faster than their hormone receptor-positive cousins and have direct involvement and implications in cell proliferation, survival, invasion and cell differentiation (6).
At the first interim analysis, DESTINY-Breast03 confirmed statistically meaningful progression-free survival (PFS) with T-DXd vs TDM-1 (7). This trial was designed as an open-label, multicentre, phase 3, randomised controlled trial to assess the safety and efficacy of T-DXd vs TDM-1 in HER2 positive, metastatic and unresectable patients who had progressed on standard therapy, which involved trastuzumab with a taxane or had progressed after completion of adjuvant or neoadjuvant therapy (> six months post this time point).
Patients were then randomised 1:1 to receive the intervention drug or TDM-1. Inclusion criteria included patients who had previously treated or had stable metastasis, confirmed HER2 positive metastatic or unresectable mBC, had received prior required therapy,
Trial Design:

Ref: https://clinicaloptions.com/CE-CME/oncology/destiny-breast03/100003032
Results:
Patients were recruited from mid-2018 to mid-2020, and 699 individuals were screened, confirming 524 patients having HER-2 positive cancer fitting the enrollment criteria and randomised 1:1 to each arm. Baseline characteristics were similar between both the arms, with the median age being 54.3 years in the T-DXd group and 54.2 years in the TDM-1. The majority of patients had an ECOG performance status of 0, with TDM-1 having a slightly higher percentage (66.5% vs 59%). Baseline Central Nervous System (CNS) metastatic disease was confirmed in 16.5% of T-DXd and 14.8% in TDM-1. Both groups had received at least two prior lines of therapy. 19.5% of patients remained on T-DXd vs 3.8% in the TDM-1 cohort as of Nov 2023. Discontinuation occurred predominantly due to disease progression followed by adverse events and then withdrawal of the patient.
The median follow-up time was 43 months or T-DXd and 35.4 for TDM-1. ORR was confirmed in 78.9% of T-DXd patients and 36.9% of TDM-1. Complete responses were observed in 12.6% vs 4.2% favouring T-DXd again. The median duration of response was 30.5 months in T-DXd and 17.0 months with TDM-1
mPFS was already reported, but we will discuss it again here, which was 29.0 months with T-DXd and 7.2 months with TDM-1. At the 36-month mark, just under half (45.7%) of T-DXd and slightly over 1/10th (12.4% of TDM-1 continued to have progression-free survival.
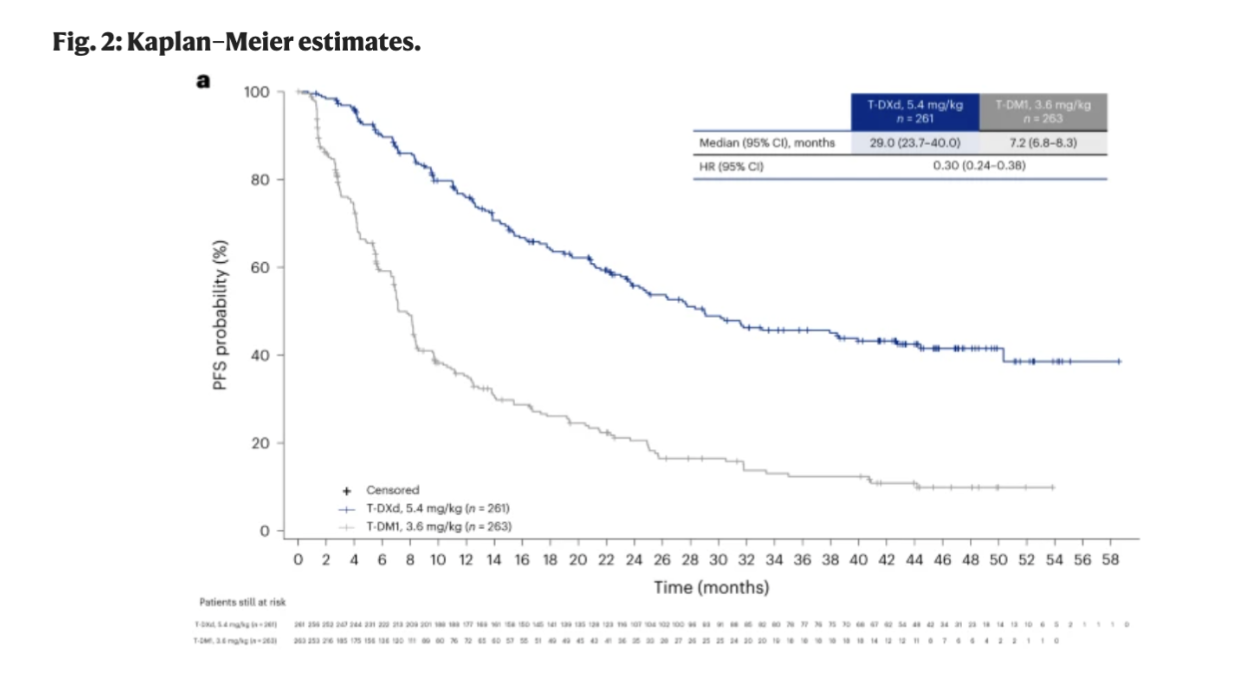
Source: https://www.nature.com/articles/s41591-024-03021-7#Fig2
The Juicy Part:
As of data cutoff from 20th November 2023, 42.1% of T-DXd and 47.9% of TDM-1 group had OS events. Median OS was 52.6 months with T-DXd vs 42.9 months TDM-1 corresponding to a reduction in death risk by 27% (HR, 0.73; 95% CI, 0.56–0.94). AT 24 months OS was 77.5% with T-DXd vs 70.1% with TDM-1 and the corresponding 36 month OS was 67.6% vs 55.7% respectivly.

Source: https://www.nature.com/articles/s41591-024-03021-7#Fig2
Toxicity:
Adverse events remain an ongoing challenge in the antibody-drug conjugate space. While efficacy across the board for many cancers has improved, this sometimes comes at a cost of further toxicity and quality of life. There were similar rates of treatment-emergent adverse events in both groups, 99.6% in T-DXd and 95.4% in the T-DM1 cohort. Adverse events greater than grade 3 were observed in 58% of T-DXd and 52.1% with T-DM1. The majority of these events were drug-related and led to discontinuation in 22.6% of the T-DXd and 7.3% in the T-DM1. The most likely adverse event associated with cessation of the drugs was pneumonitis in T-DXd, and for T-DM1, this was also found in 1.5% of patients and further issue of thrombocytopenia. Stringent guidelines exist for T-DXd concerning identifying pneumonitis and mitigating the risk of this causing mortality or significant morbidity.
Discussion and Conclusion:
We continue to see efficacy in the T-DXd cohort to both effectiveness, objective response rate and median overall survival showed an approximate ten month improvement over T-DM1 with reduction in the risk of death by 27%. Compared to the EMILIA trial, the median OS was much longer in this trial when comparing TDM-1 arms (42.7 months s 29.9 months). The nature of cross-trial comparisons should never be considered gospel, given the difference between each trial and each patient cohort. Crossover was not a component of this trial, but post-progression, many patients had subsequent anti-HER2 therapy, including T-DM1, T-DXd, pertuzumab and other tyrosine kinase inhibitors, which could impact the readout of the OS in both arms. A third of the T-DM1 arm had T-DXd as their following line in therapy.
In summary, TDX-d offers an effective, second-line therapy for patients progressing on first-line treatment. There is improvement in the objective response rate, progression-free survival, and overall survival. Like many treatments, there continue to be challenges regarding toxicity and how to best mitigate this for the patients. Other unanswered questions remain, including how to mitigate resistance, optimise patient dosing, and sequence further therapies as new drugs emerge.
Reference